This is an acronym adopted by many practitioners as an umbrella term for lip, tongue, and buccal-ties.
An individual can possess multiple ties from 3 locations including the tongue, lip, and cheek.
The term you will see often is ankyloglossia. Ankylo means (stiff, fused, fixed), and glossia means (tongue). Ankyloglossia is also known as tongue tie, which is a congenital (born with it) oral anomaly that may decrease the mobility of the tongue and is caused by an unusually short, thick lingual frenulum, a membrane connecting the underside of the tongue to the floor of the mouth.
Frenulum: A small frenum. The terms “frenum” and “frenulum” are often interchanged.
Frenum: This is the general term given to any fold, band of tissue, or mucus membrane in the body that attaches or anchors to a semi-mobile organ in the body. The connective tissue holds oral soft tissue in place against the jaw and skull bones. These tissues are created during fetal development, and in most cases, the growing baby’s frenum gradually reduces in size, a process known as apoptosis allowing for necessary mouth movement prior to birth. However, some infants are born with these tissues enlarged, hardened, or immobile. Which may lead to the removal of some frenum tissue. You may see the word written as either frenum or frenulum. Both are technically correct, which can be a little confusing. However, the plural form is likely to be more confusing, since there are three acceptable plural forms: frenulums, frenula, and frena. All of these varied spellings and plural forms refer to the same tissue.
Like the tissue itself, the procedure to reduce the connective tissues and allow for freer movement of the lips, tongue, and mouth is known by many names. You may see frenectomy, frenotomy, or frenulectomy used interchangeably. All three refer to procedures that release the soft tissue from the harder bone tissues. This can be performed using a number of different techniques, but most often, dentists or oral surgeons will perform a frenectomy using surgical scissors, lasers, or a combination of the two.

While the term “tongue and lip tie” is beginning to become more common, there are still many components that are misunderstood. One such example is identification.
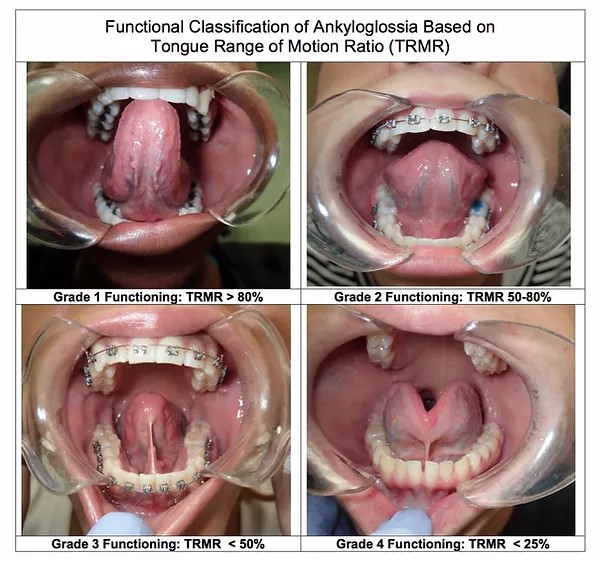
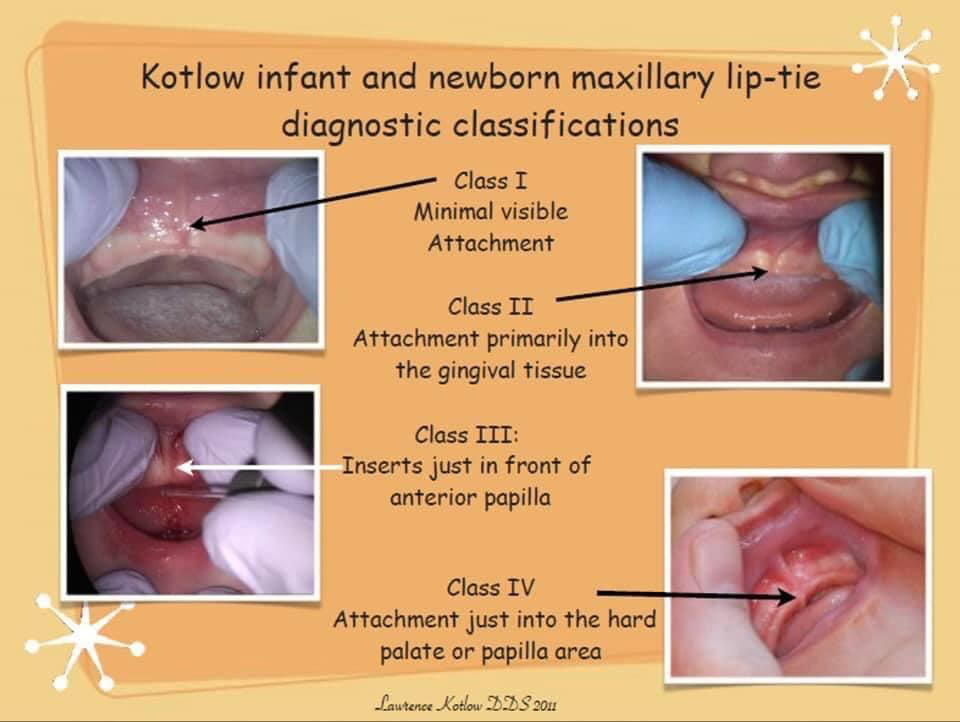
Dr. Larry Kotlow, a pediatric dentist and one of the leading experts in Tethered Oral Tissues (TOT’s), has devised a classification system based on the location of where a tie attaches, that many (but not all) TOTs experts use. However, this is not a classification of severity, but location only.
Classes 1 and 2 are anterior tongue ties. Classes 3 and 4 are posterior tongue ties.
Anterior Tongue Ties: This type of tongue-tie is very much visible and most commonly detected. These visible flaps of tissue attach to the tip, middle, or base of the tongue to the floor of the mouth.
● It is either at the tip of the tongue (Class 1) (sometimes resulting in a heart-shaped tongue tip) or, just behind the tip of the tongue (Class 2).
● Class 1 ties are usually the only ones that some medical professionals consider a “real” tie, leading to many parents’ concerns being dismissed. However, some leading experts feel that every anterior tie also has a posterior component to it as well.
Posterior Tongue Ties: This type of restriction is under the tongue and not as easily identified. These are “hidden” ties, generally beneath the mucous membrane, and need to be felt in order to be diagnosed. Sometimes a child is observed as having a “short tongue” when in actuality there is a posterior tongue tie.
● Here the membrane is less visible (Class 3), or hidden completely (Class 4).
● It is under the tongue and in the case with Class 4s, needs to be gently pushed down at the base and sides to be seen.
● Unless a health professional has specific training in tie identification, posterior tongue ties are most often missed.